The goal of the North Coast Quality Improvement Network is to build capacity of Network health centers to make data driven decisions to improve the overall population health of our rural communities, to improve patient experience, and to better control health care costs.
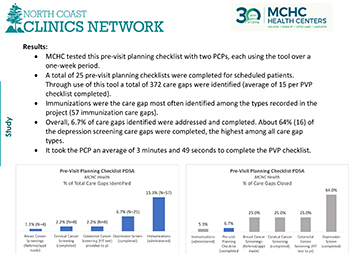
MCHC Health Centers Pre-Visit Planning Checklist
Aim: Aim: By 9/21/22, MCHC will complete the pre-visit planning checklist for at least 25 patients.
Measures:
Outcome Measures:
• % of care gaps closed
Process Measures:
• of pre-visit planning checklists completed
• # of care gaps identified
• # of minutes to complete the pre-visit planning checklist
Read more here!
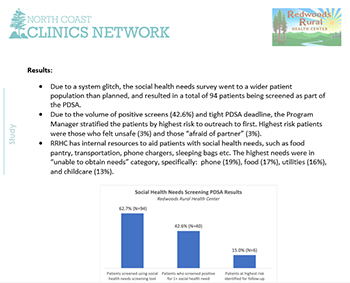
Redwoods Rural Health Center Social Determinants of Health Screening
Aim: By 9/20/2022, Redwoods Rural Health Center will select a social health needs screening tool, screen 20 patients, and refer them to social needs resources.
Measures:
Outcome Measures:
• % of patients screened who screen positive for social health needs
• % of patients who screen positive that accept social health needs referral
Process Measures:
• % of patients identified to be screened who consent and are screened for social health needs
• % of patients who screen positive that are at highest risk (stratify for outreach)
Read more here!
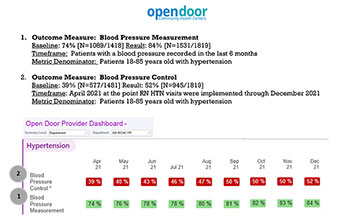
Open Door Community Health Centers (ODCHC) Improve Blood Pressure Control for Patients (HTN)
Aim: Pilot implementation of RN Hypertension visits following a protocol with recommendations from the American Medical Associations (AMA) BP MAP Program, to provide follow up visits with patients starting new hypertension medications.
- Outcome Measure: The percent of hypertensive patients for whom the last BP measurement at an ambulatory care visit were at goal, defined as systolic BP (SBP) < 140 mmHg and diastolic BP (DBP) < 90 mmHg (NQF 0018);
- Outcome Measure: The percentage of hypertensive patients with a BP measurement recorded in the last 6 months;
- Process Measure: The number of RN Hypertension visits that have taken place at pilot site.
- Process Measure: The percent of times a second BP measurement was recorded in the same visit when the first measurement was over target (SBP ≥ 140 mmHg or DBP ≥ 90 mmHg);
- Read more here!
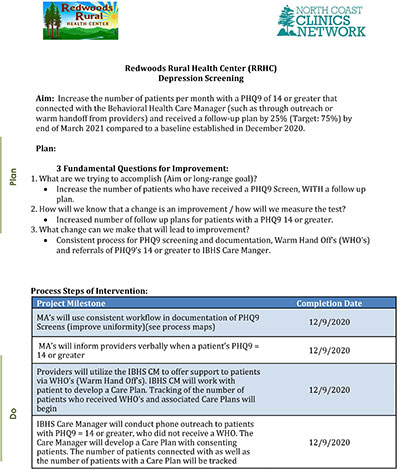
Redwoods Rural Health Center (RRHC) Depression Screening
Aim: Increase the number of patients per month with a PHQ9 of 14 or greater that connected with the Behavioral Health Care Manager (such as through outreach or warm handoff from providers) and received a follow-up plan by 25% (Target: 75%) by end of March 2021 compared to a baseline established in December 2020.
3 Fundamental Questions for Improvement:
- What are we trying to accomplish (Aim or long-range goal)?
• Increase the number of patients who have received a PHQ9 Screen, WITH a follow up plan. - How will we know that a change is an improvement / how will we measure the test?
• Increased number of follow up plans for patients with a PHQ9 14 or greater. - What change can we make that will lead to improvement?
• Consistent process for PHQ9 screening and documentation, Warm Hand Off’s (WHO’s) and referrals of PHQ9’s 14 or greater to IBHS Care Manger.
Childhood IZ Story Board
Aim: Open Door Community Health Centers’ Eureka Community Health Center (ECHC) will increase the rate of children aged 0‐2 who were fully immunized from 31.84% to 34.79%, the 50th Percentile for Partnership HealthPlan of California’s 2020 Quality Improvement Program.
Measure:
* Outcome Measure: % of children aged 0‐2 who were fully immunized by their 2nd birthday; * Process Measures: % of patients who did not show for their immunizations; average cycle time
Read more here!

Open Door Community Health Centers (ODCHC) Well Child Group Visits
Aim: Open Door Community Health Centers’ Eureka Community Health Center (ECHC) will increase the rate of children aged 3-6 who had a Well Child Visit (WCV) from 75.4% to 83.7%, the 90th Percentile for Partnership HealthPlan of California’s 2019 Quality Improvement Program.
Measures:
• Outcome Measure: % of children aged 3-6 who received one or more Well Child Visits with a PCP during the measurement year;
• Process Measures: % of patients who did not show for their WCV; % of patients who cancelled; average cycle time; patient and staff satisfaction.
Read more here!

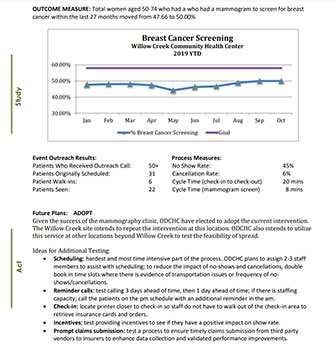
Mobile Mammography Event
Aim: Open Door Community Health Centers’ Willow Creek Community Health Center (WCCHC) will increase the rate of women aged 50-74 who had a mammogram to screen for breast cancer from 47.66% to 58.04%, the 50th Percentile for Partnership HealthPlan of California’s 2019 Quality Improvement Program.
Measures:
• Outcome Measure: % of women aged 50-74 who had a mammogram to screen for breast cancer within the last 27 months; • Process Measures: % of patients who did not show for their mammogram; % of patients who cancelled; average cycle time; % of mammograms requiring additional screening.
Read more here!